

Introduction:
ES after autoHCT encompasses a continuum of peri-engraftment complications characterized by non-infectious fever, rash, diarrhea, and capillary leak features. ES is an increasingly recognized complication after autoHCT in MM, with the varying incidence reported, based on the diagnostic criteria used. ES is typically mild and self-limited in most patients, while a subset can develop severe complications. In this study, we explored whether the use of budesonide prophylaxis reduces ES rates in MM patients undergoing autoHCT.
Methods:
All patients who underwent autoHCT for MM from 12/2017 to 11/2019 were included after IRB approval at our institution. Beginning on 12/15/2018, as a quality improvement institutional initiative to reduce ES, budesonide 3 mg orally three times a day was initiated at day +5 post autoHCT and continued until the time of discharge. In patients developing ES, systemic steroids were started, and budesonide was discontinued. The efficacy of the intervention was compared with patients who did not receive prophylaxis prior to the study period. ES was defined according to the previously published criteria [T R Spitzer BMT 50, 469-475(2015)]. Patient demographics, disease, and treatment outcomes between the 2 groups were compared using Mann-Whitney and Chi-squared tests when appropriate. The primary outcome was the ES rates between the 2 groups. Multiple logistic regression was used to model ES rates with other predictors, including budesonide prophylaxis as the main effect. Length of stay (LOS) and 30-day readmission were the secondary endpoints.
Results:
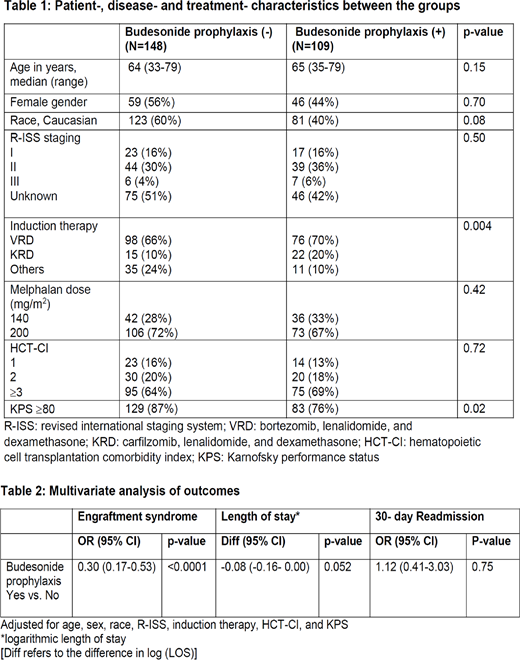
Table 1 shows the patient-, disease- and treatment characteristics between no prophylaxis (N=148) and prophylaxis (N=109) groups. The two groups were well matched overall except for induction therapy and Karnofsky performance status (KPS). The rates of ES were significantly higher in the no prophylaxis group vs. prophylaxis group [69 (75%) vs. 23 (25%); p<0.001]. All patients in both groups were able to achieve neutrophil and platelet engraftment at day 28 and day 100, respectively. There was no significant difference in LOS [mean 15 (±3.2) vs. 16 (±2.8); p=0.27] and 30-day readmission [9 (6%) vs. 8 (7%); p=0.81] between the no prophylaxis and prophylaxis groups, respectively.
On adjusted analysis, budesonide prophylaxis was associated with a significantly lower risk of developing ES compared to no prophylaxis groups [Odds ratio, OR 0.30 (95%CI: 0.17-0.53); p<0.0001]. No other significant predictors were identified for the development of ES. There was no difference in the 30-day readmission rates [OR 1.12 (95%CI: 0.41-3.03); p= 0.75], but a trend for shorter LOS in the prophylaxis group [7.3% reduction in LOS (95%CI: 14.4%- 0%); p=0.052] (Table 2).
Conclusion:
Our study concludes that the use of budesonide prophylaxis significantly reduces the risk of ES in MM patients undergoing autoHCT. Future large-scale randomized studies are needed to confirm these findings in patients undergoing autoHCT for MM and other diseases.
Dhakal:Celgene: Consultancy, Honoraria; Takeda: Consultancy, Other: Advisory Board; Sanofi: Research Funding; Amgen: Consultancy, Other: AdvIsory Board, Research Funding; Janssen: Consultancy, Other: Advisory Board, Research Funding; GSK: Consultancy, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal